
Severe Hyperkalemia: Electrocardiographic Tips for Early Recognition Based on a Case Report
DOI:
https://doi.org/10.5195/ijms.2024.1907Keywords:
Hyperkalemia, Electrocardiography, Potassium, Renal Insufficiency, Acute, Metabolic Acidosis, Cardiorespiratory Arrest, Myocardial Infarction, Coronary Angioplasty, Ejection Fraction, Hypertension, Dyslipidemias, Atrial Fibrillation, Diabetes Mellitus, Type 2, Asthenia, Dyspnea, Insulin, Diuretics, Acid-Base Imbalance, Ventricular Function, Left, Emergency TreatmentAbstract
Background: Rapid correction of severe hyperkalemia is mandatory to survival due to its induction of fatal cardiac arrhythmias. The electrocardiogram serves as the diagnostic tool that can provide insight into such fatal arrhythmias. We present two relevant alterations seen in an 84-year-old female patient with previous anterior myocardial infarction, angioplasty of the circumflex coronary artery, left ventricular ejection fraction of 35%, hypertension, dyslipidemia, paroxysmal atrial fibrillation, and diabetes.
The Case: The patient had 4-days with asthenia, adynamia and dyspnea. Lung auscultation showed bilateral base rales with cardiomegaly and interstitial edema identified on chest x-ray. Lab work revealed severe metabolic acidosis, increased plasma urea, creatinine, and severe hyperkalemia (7.9 mEq/liter) considered secondary to acute renal failure. Treatment was initiated with 0.9% sodium chloride, bicarbonate, ASA diuretics and polarizing solution (insulin), resulting in a reduction of hyperkalemia to 6.1 mEq/liter. The patient suffered a cardiorespiratory arrest with recovery and needed intubation and dopamine for hemodynamic support but died 15 hours after admission.
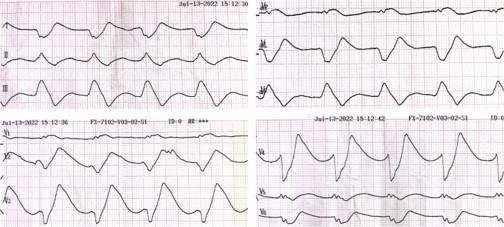
Conclusion: The electrocardiographic findings characteristic of severe hyperkalemia were: (i) regular rhythm (cycle length 920-950 ms) without discernible P-waves, which may have a junctional or ventricular origin and less probably could be a manifestation of sinoventricular conduction (preferential conduction from the sinus node to the AV node through specialized tracts without activation of the atrial cardiomyocytes), and (ii) sine wave morphology (markedly wide QRS, absence of ST-segment and broadly based T-waves). These electrocardiographic features, typical of hyperkalemia exceeding 7.0 mEq/liter, are harbingers of malignant arrhythmias and should prompt immediate therapy.
References
Palmer BF, Clegg DJ. Physiology and pathophysiology of potassium homeostasis. Adv Physiol Educ. 2016; 40 (4):480-90.
Chou T-C, Knilans TK. Electrocardiography in clinical practice. Adult and pediatric. 4th ed. Philadelphia: W. B. Saunders; 1996.
Weiss JN, Qu Z, Shivkumar K. The electrophysiology of hypo- and hyperkalemia. Circ Arrhythm Electrophysiol. 2017; 10 (3):e004667
Montford JR, Linas S. How dangerous is hyperkalemia? J Am Soc Nephrol. 2017; 28 (11):3155-65.
Durfey N, Lehnhof B, Bergeson A, Durfey SNM, Leytin V, McAteer K, et al. Severe hyperkalemia: Can the eElectrocardiogram risk stratify for short-term adverse events? West J Emerg Med. 2017;18(5):963-71.
Levine HD, Wanzer SH, Merrill JP. Dialyzable currents of injury in potassium intoxication resembling acute myocardial infarction or pericarditis. Circulation. 1956; 13 (1):29-36.
Gottschalk BH, Anselm DD, Benditt DG, Makeshwari A, Sreenivasan S, Abu Shama R, et al. Relation of the Brugada phenocopy to hyperkalemia (from the International Registry on Brugada phenocopy). Am J Cardiol. 2018; 121 (6):715-17.
Sherf L, James TN. A new electrocardiographic concept: Synchronized sinoventricular conduction. Dis Chest. 1969; 55 (2):127-40.
Vassale M, Hoffman BF. The spread of sinus activation during potassium administration. Circ Res. 1965; 17 (4):285-95.
Maradey J, Bhave P. Sinoventricular conduction in the setting of severe hyperkalemia. JACC Clin Electrophysiol. 2018; 4 (5):701-3.
Published
How to Cite
Issue
Section
Categories
License
Copyright (c) 2024 Patricio I. Frangi , Jorge Gonzalez-Zuelgaray, Luisina B. Tosoni, Adrian Baranchuk

This work is licensed under a Creative Commons Attribution 4.0 International License.
Authors who publish with this journal agree to the following terms:
- The Author retains copyright in the Work, where the term “Work” shall include all digital objects that may result in subsequent electronic publication or distribution.
- Upon acceptance of the Work, the author shall grant to the Publisher the right of first publication of the Work.
- The Author shall grant to the Publisher and its agents the nonexclusive perpetual right and license to publish, archive, and make accessible the Work in whole or in part in all forms of media now or hereafter known under a Creative Commons Attribution 4.0 International License or its equivalent, which, for the avoidance of doubt, allows others to copy, distribute, and transmit the Work under the following conditions:
- Attribution—other users must attribute the Work in the manner specified by the author as indicated on the journal Web site; with the understanding that the above condition can be waived with permission from the Author and that where the Work or any of its elements is in the public domain under applicable law, that status is in no way affected by the license.
- The Author is able to enter into separate, additional contractual arrangements for the nonexclusive distribution of the journal's published version of the Work (e.g., post it to an institutional repository or publish it in a book), as long as there is provided in the document an acknowledgment of its initial publication in this journal.
- Authors are permitted and encouraged to post online a prepublication manuscript (but not the Publisher’s final formatted PDF version of the Work) in institutional repositories or on their Websites prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work. Any such posting made before acceptance and publication of the Work shall be updated upon publication to include a reference to the Publisher-assigned DOI (Digital Object Identifier) and a link to the online abstract for the final published Work in the Journal.
- Upon Publisher’s request, the Author agrees to furnish promptly to Publisher, at the Author’s own expense, written evidence of the permissions, licenses, and consents for use of third-party material included within the Work, except as determined by Publisher to be covered by the principles of Fair Use.
- The Author represents and warrants that:
- the Work is the Author’s original work;
- the Author has not transferred, and will not transfer, exclusive rights in the Work to any third party;
- the Work is not pending review or under consideration by another publisher;
- the Work has not previously been published;
- the Work contains no misrepresentation or infringement of the Work or property of other authors or third parties; and
- the Work contains no libel, invasion of privacy, or other unlawful matter.
- The Author agrees to indemnify and hold Publisher harmless from the Author’s breach of the representations and warranties contained in Paragraph 6 above, as well as any claim or proceeding relating to Publisher’s use and publication of any content contained in the Work, including third-party content.
Enforcement of copyright
The IJMS takes the protection of copyright very seriously.
If the IJMS discovers that you have used its copyright materials in contravention of the license above, the IJMS may bring legal proceedings against you seeking reparation and an injunction to stop you using those materials. You could also be ordered to pay legal costs.
If you become aware of any use of the IJMS' copyright materials that contravenes or may contravene the license above, please report this by email to contact@ijms.org
Infringing material
If you become aware of any material on the website that you believe infringes your or any other person's copyright, please report this by email to contact@ijms.org




